

เมื่อปลายเดือนที่ผ่านมา นักศึกษาแพทย์ในทีมวิจัยของเราได้รับการตีพิมพ์ผลงานวิจัยในวารสารแพทยศาสตรศึกษา Medical Education Online ซึ่งเป็นวารสารวิชาการระดับ Q1 ภายใต้ชื่อบทความ “Early exposure to a primary care course: a co-created transformative approach in health systems science” โดยงานชิ้นนี้นำเสนอการพัฒนาการเรียนการสอนด้านวิทยาระบบสุขภาพ† (Health Systems Science) ในหลักสูตรแพทยศาสตรบัณฑิตโดยเชื่อมโยงกับบริบทจริงของระบบสุขภาพในประเทศไทยและการดูแลปฐมภูมิ ซึ่งเป็นการเติมเต็มหลักสูตรการศึกษาของแพทย์และวิชาชีพด้านสุขภาพในบริบทประเทศรายได้ปานกลางที่ยังมีการเรียนการสอนในด้านวิทยาระบบสุขภาพอย่างจำกัด
ในช่วงทศวรรษที่ผ่านมาวิทยาระบบสุขภาพได้รับการยอมรับในฐานะ “เสาหลักที่สาม (Third Pillars)” ของการศึกษาวิทยาศาสตร์สุขภาพ ควบคู่ไปกับวิทยาศาสตร์พื้นฐาน (Basic science) และวิทยาศาสตร์คลินิก (Clinical science) เพื่อบูรณาการทักษะที่จำเป็นสำหรับการส่งมอบบริการทางสุขภาพที่มีประสิทธิภาพและเพิ่มความสามารถในการจัดการสุขภาพประชากร โดยขอบเขตความรู้วิทยาระบบสุขภาพสำหรับแพทย์ ประกอบไปด้วย
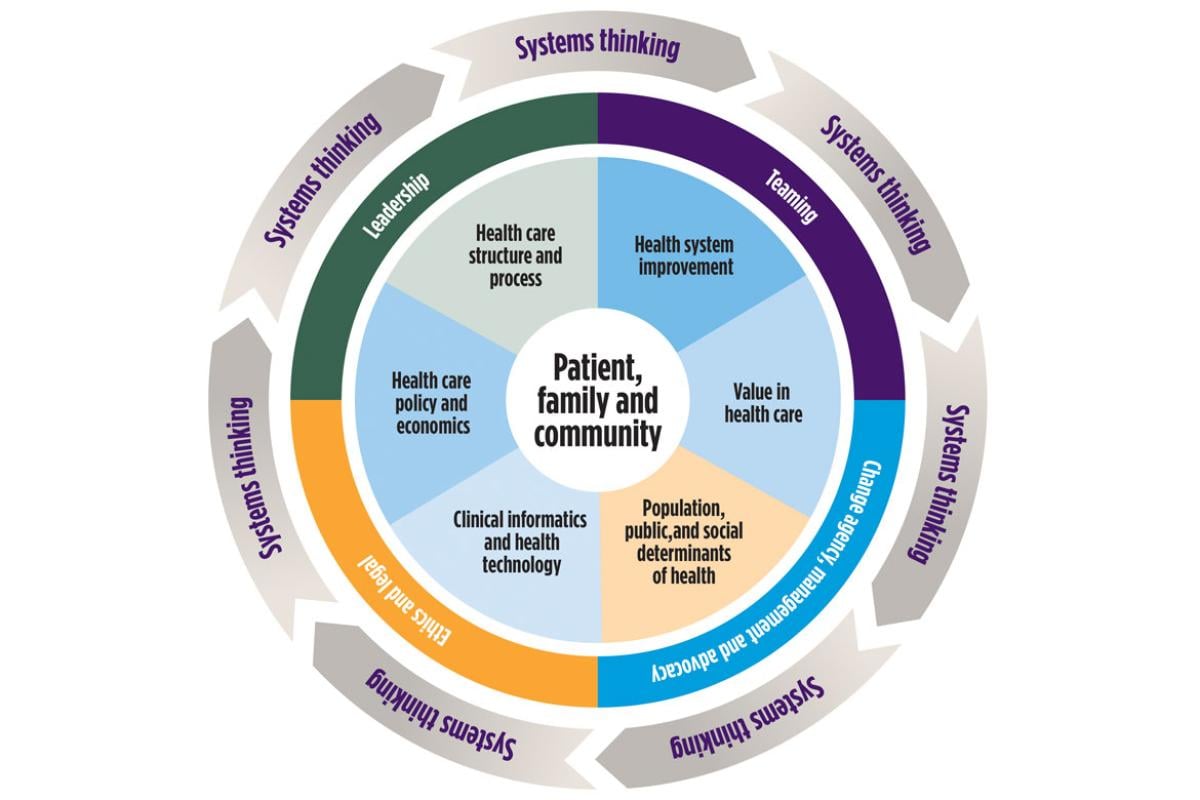
1. ขอบเขตความรู้หลัก (Core Domains) ได้แก่ โครงสร้างและกระบวนการจัดบริบาลสุขภาพ (Health care structures and processes) นโยบายการจัดบริบาลสุขภาพ เศรษฐศาสตร์สุขภาพ และการจัดการระบบบริบาลสุขภาพ (Health care policy, economics, and management) สารสนเทศคลินิกและเทคโนโลยีสารสนเทศสุขภาพ (Clinical Informatics and Health Technology) สุขภาพระดับกลุ่มประชากร (Population Health) การดูแลรักษาแบบเน้นคุณค่า (Value-based care) และการพัฒนาระบบสุขภาพ (Health system improvement)
2. ขอบเขตความรู้ข้ามประเด็น (Cross-Cutting Domains) ได้แก่ ภาวะผู้นำและการสร้างการเปลี่ยนแปลง (Leadership and change agency) การทำงานเป็นทีมและการศึกษาแบบสหวิชาชีพ (Teamwork and interprofessional education) การปฏิบัติตามหลักฐานและสารสนเทศ (Evidence-based medicine and practice) ความเป็นมืออาชีพและจริยธรรมวิชาชีพ (Professionalism and ethics) ความเป็นนักวิชาการ (Scholarship)
3. ขอบเขตความรู้เชื่อมโยงประเด็น (Linking Domains) ได้แก่ การคิดเชิงระบบ (Systems Thinking)
อย่างไรก็ดี ที่ผ่านมาการบูรณาการวิทยาระบบสุขภาพเข้ากับแพทยศาสตรศึกษายังเป็นไปอย่างล่าช้าและแยกส่วน เนื่องจากการรับรู้ความซับซ้อนที่แตกต่างกันในแต่ละภาคส่วน จำนวนผู้เชี่ยวชาญที่มีอยู่อย่างจำกัด และการวางแผนหลักสูตรที่มักประสบกับความไม่แน่นอนต่าง ๆ
การศึกษาวิจัยนี้เสนอการออกแบบกิจกรรมของหลักสูตรที่บูรณาการวิทยาระบบสุขภาพผ่านกระบวนการมีส่วนร่วมในการออกแบบการเรียนรู้ของ 4 ภาคส่วน ได้แก่นักศึกษาแพทย์ อาจารย์ผู้ดูแลแพทยศาสตร์ศึกษา อาจารย์ด้านวิทยาระบบสุขภาพ และผู้บริหารโรงพยาบาลชุมชน 4 โรงพยาบาล โดยรูปแบบกิจกรรมเกิดขึ้นก่อนเปิดภาคเรียนชั้นปีที่ 1 และปีที่ 2 ของนักศึกษาแพทย์ โครงสร้างการเรียนรู้ประกอบด้วย (1) การเรียนการสอนที่เน้นการมีส่วนร่วม (Interactive Class) (2) การออกภาคสนามในโรงพยาบาลชุมชนและชุมชนในพื้นที่ (3) การทำโครงการขนาดเล็กภายหลังจากการออกภาคสนาม และ (4) ภายหลังกิจกรรมต่าง ๆ นักศึกษาที่เข้าร่วมจะประเมินการศึกษาของตนเองผ่านกระบวนการเขียนสะท้อนคิด (reflective writing) ตลอดจนการวางแผนการเรียนรู้ในอนาคต
ผลจากการศึกษาพบว่า กระบวนการที่จัดขึ้นนั้นนำไปสู่การเรียนรู้เชิงเปลี่ยนแปลง (transformative learning) ผ่านกลไก “ประสบการณ์–การสะท้อน–ความเชื่อมั่น” (Exposure-Transformation-Self Efficacy) ทีมผู้วิจัยพบว่าการเปิดโอกาสให้นักศึกษาได้เผชิญกับสถานการณ์จริงที่สะท้อนช่องว่างและปัญหาของระบบสุขภาพในบริบทของคนหน้างานนั้นมีบทบาทสำคัญในการกระตุ้นกระบวนการเรียนรู้ผ่านการเผชิญหน้ากับภาวะความยากลำบากในสถานการณ์จริง (authentic dilemmas) ช่วยกระตุ้นการสะท้อนคิดเชิงวิพากษ์ ส่งผลให้มุมมองของผู้เรียนต่อการเรียนรู้นั้นเกิดการเปลี่ยนแปลง และเสริมสร้างการรับรู้ถึงความสามารถของตนเอง (perceived self-efficacy) เมื่อความเชื่อมั่นของนักศึกษาเพิ่มขึ้น ผู้เรียนมีแนวโน้มที่จะแสวงหาประสบการณ์การเรียนรู้เพิ่มเติม และมีส่วนร่วมในการเสนอแนวคิดใหม่ ๆ ต่อการออกแบบการเรียนรู้ ซึ่งช่วยเสริมพลัง (empowerment) และการตั้งใจที่มีเข้ามามีส่วนร่วมในการเรียนรู้ (engagement) ไปพร้อมกัน
ในท้ายที่สุดแล้ว การศึกษานี้ต้องการชี้ให้เห็นว่า การจัดการเรียนรู้ในวิทยาระบบสุขภาพ หากได้รับการออกแบบโดยเปิดพื้นที่ให้ผู้เรียนมีส่วนร่วมในฐานะผู้ร่วมสร้างการเรียนรู้ ย่อมสามารถพัฒนาความเข้าใจเชิงระบบของนักศึกษาได้อย่างมีความหมายมากกว่าการถ่ายทอดความรู้เชิงทฤษฎีเพียงอย่างเดียว และหัวใจของคุณค่าทางการศึกษาของหลักสูตรนี้อยู่ที่การที่นักศึกษาได้มีส่วนร่วมอย่างต่อเนื่องกับการปฏิบัติงานจริงในระบบบริการปฐมภูมิ บริบทของชุมชน และการเผชิญกับปัญหาเชิงระบบในชีวิตจริง ผ่านการเปลี่ยนแปลงกระบวนทัศน์ (Paradigm shift) ของการศึกษาทางการแพทย์ไปสู่การศึกษาที่มีความรับผิดชอบต่อสังคม (Social accountable education) อย่างเป็นรูปธรรม การบูรณาการการประสบการณ์การเรียนรู้จากบริบทจริงเข้ากับหลักสูตรตั้งแต่ช่วงต้นของการเรียน จึงอาจเป็นก้าวสำคัญในการเตรียมแพทย์ที่ไม่เพียง “รักษาโรค” แต่สามารถเข้าใจและโอบรับความซับซ้อนของระบบสุขภาพ ร่วมออกแบบ และร่วมพัฒนาระบบสุขภาพที่มีคุณภาพ เป็นธรรม และยั่งยืนในระยะยาว
คณะผู้วิจัยขอขอบพระคุณท่านอดีตคณบดีคณะแพทยศาสตร์ โรงพยาบาลรามาธิบดี มหาวิทยาลัย ศาสตราจารย์ นายแพทย์ปิยะมิตร ศรีธรา ที่สนับสนุนให้โครงการนี้เกิดขึ้นจริง และนักศึกษาแพทย์ทุกท่านที่ตั้งใจร่วมออกแบบ เรียนรู้ และประเมินโครงการนี้ และหวังว่าจะมีผลงานทั้งในเชิงงานวิจัยและความวิจัยจากโครงการนี้ที่ได้ขยายผลไปยังรุ่นต่อไป
หากสนใจอ่านเพิ่มเติมสามารถเข้าไปอ่านบทความที่ตีพิมพ์ฉบับเต็มในวาสาร Medical Education Online ได้ที่นี่ ผลงานตีพิมพ์ในลักษณะ Open Access ซึ่งทุกท่านสามารถอ่าน บันทึก แชร์บทความวิจัยได้โดยไม่มีค่าใช้จ่าย
In late last month, a medical student in our research team published a research article in Medical Education Online, a Q1-ranked medical education journal. The article, titled “Early exposure to a primary care course: a co-created transformative approach in health systems science,” presents the development of teaching and learning in Health Systems Science (HSS) within the medical curriculum. The study links HSS education to the real-world context of Thailand’s health system and primary care practice. It contributes to strengthening medical and health professions education in middle-income country settings, where formal training in HSS remains limited.
Over the past decade, HSS has been increasingly recognized as the “third pillar” of health professions education, alongside basic science and clinical science. Its purpose is to integrate the competencies required for effective health service delivery and to enhance the capacity to manage population health. HSS encompasses several domains:
1. Core Domains including Health care structures and processes, Health care policy, economics, and management, Clinical Informatics and Health Technology, Population Health, Value-based care, and Health system improvement
2. Cross-Cutting Domains including Leadership and change agency, Teamwork and interprofessional education, Evidence-based medicine and practice, Professionalism and ethics, and Scholarship
3. Linking Domains which is Systems Thinking
Despite this growing recognition, the integration of Health Systems Science into medical education has remained slow and fragmented. This has been attributed to differing perceptions of system complexity across stakeholders, a limited pool of subject-matter experts, and persistent uncertainties in curriculum design and implementation.
This study proposes a curriculum activity design that integrates HSS through a participatory co-design approach involving four key stakeholder groups: medical students, medical education faculties, HSS faculties, and directors from four community hospitals. The learning activities were implemented prior to the start of the first- and second-year medical curricula. The learning structure comprised four components: (1) interactive, participatory classroom sessions; (2) field-based learning in community hospitals and surrounding communities; (3) mini-project development following the fieldwork; and (4) post-activity self-assessment through reflective writing, in which participating students critically reflected on their learning experiences and formulated plans for future learning.
The findings indicate that the implemented process facilitated transformative learning through an “Exposure–Transformation–Self-Efficacy” mechanism. Providing students with opportunities to engage directly with real-world situations that revealed gaps and challenges within the health systems, as experienced by frontline practitioners, played a critical role in activating learning processes. Confrontation with authentic dilemmas in real practice settings stimulated critical reflection, leading to shifts in learners’ perspectives on learning and strengthening their perceived self-efficacy. As students’ confidence increased, they became more inclined to seek additional learning experiences and to contribute new ideas to the design of learning activities. This process simultaneously fostered empowerment and deeper engagement in learning.
Finally, this study highlights that learning in HSS, when intentionally designed to position learners as co-creators of knowledge, can foster a more meaningful and robust systems understanding than theoretical knowledge pedagogy alone. The core educational value of this curriculum lies in students’ sustained engagement with real-world practice in primary care settings, community contexts, and the lived experience of systemic challenges within health systems. Through a paradigm shift in medical education toward concretely enacted social accountability, the integration of experiential learning grounded in real-world contexts from the early stages of training may represent a critical step in preparing future physicians who not only “manage disease,” but also understand, embrace, and engage with the complexity of health systems. Such an approach enables learners to participate in the co-design and continuous improvement of health systems that are high-quality, equitable, and sustainable in the long term.
The research team would like to express our sincere gratitude to the former Dean of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Professor Piyamitr Sritara, MD, for his support in making this project possible. We also extend our appreciation to all medical students who actively participated in the co-design, learning, and evaluation of this project. We hope that both research outputs and practice-based insights emerging from this initiative will continue to be developed and extended to future cohorts.
For those interested in further reading, the full published article is available in Medical Education Online The article is published as Open Access, allowing readers to freely access, save, and share the research without any charge.
†
คำแปลทางการของ Health Systems Science เป็นภาษาไทยนั้นยังไม่มีข้อยุติ หากพิจารณาโดยหลักการของราชบัณฑิตยสภาอาจสามารถแปลได้ว่าอย่าง “ระบบสุขภาพศาสตร์” ตามลักษณะของรัฐศาสตร์ (Political Science) สังคมศาสตร์ (Social Science) หรือเศรษฐศาสตร์ (Economic Science) ซึ่ง “ศาสตร์” ในที่นี้หมายความถึงระบบความรู้หรือระบบปัญญาที่มีกรอบคิดและวิธีวิทยาเฉพาะ หรือแปลได้ว่า “วิทยา(การ)ระบบสุขภาพ” ตามลักษณะของวิทยาการข้อมูล (Data Science) หรือวิทยาการคอมพิวเตอร์ (Computer Science) ซึ่ง “วิทยาการ” ในที่นี่หมายความถึงการนำความรู้จากหลากหลายศาสตรมาใช้ในการแก้ปัญหาหรือระบบ ซึ่งมีลักษณะของศาสตร์ประยุกต์มากกว่า อย่างไรเสีย ในงานชิ้นนี้ ผู้เขียนจะใช้ “วิทยาระบบสุขภาพ” ในลักษณะศาสตร์เชิงประยุกต์สำหรับการแก้ปัญหาเชิงระบบในระบบสุขภาพ